


Low Dose Naltrexone: The Chronic Pain Management Option 90% Doctors Don’t know About

Chronic pain is an invisible disability. Yes, it hurts, but it also causes a host of debilitating and heartbreaking issues. From a mental standpoint, it become hard to concentrate. Brain fog and mental exhaustion become the new norm, not to mention the grouchiness. Of course you’re grouchy! You’re sick of hurting all of the time. And then there is the guilt, your constant companion. You’re continually judging yourself thinking about how you should be. On some days, the pain can take so much out of you that even small tasks can take a monumental effort. It’s tragic really, and its effects on your life are hard to put into words. People without chronic pain can’t even begin to fathom all of the subtle changes and the toll it has taken on your life. It changes everything.
We know that the last thing you want to hear about is another solution. We’re sure you’ve probably already tried everything under the sun to get better. You’ve most likely also been to all of the pain management doctors for 2nd, 3rd and even 4th opinions. But frankly, we’re here to tell you that none of that matters. Conventional medicine can only go so far. We’re here to offer you some hope.
At Harbor Compounding Pharmacy we take what we do seriously. We try to be on the cutting edge of research and disease management. For our pharmacists, it’s starts with learning about the latest in what is actually causing the disease. We don’t simply rely on what was taught to us in school and what the medicals norm are. There is so much information and published research out there. You can think of us your conduit to help you get the results you’re looking for, especially when there is no one left to help. When we’re looking for an alternative solution, it’s important to us that we find a safe, effective and researched treatment options. We’re not okay with fixing one thing and causing another problem - and while we’re conducting our research, we’re always looking for solutions that get to the root of the problem.
And since we’re drug formulators, we’re able to bring the unique solutions we find to life. We are meticulous in our formulation development so that our recommendations can make a truly impactful difference in the lives of the people we try to help – like you. Read on and we promise to share a detailed description of how low dose naltrexone works, as well as the studies that we have found to help you with your decision on how you would like to treat your chronic pain.
The people who show up to a doctor’s office in pain typically show up for 1 of 2 main reasons. The first reason, which we can all most likely relate to, is a sudden onset of pain. It’s typically caused by an injury like a gash or a broken arm. And when that injury has healed, the pain retreats and eventually disappears. This is known as acute pain.
The other type of pain usually progresses slowly. Maybe over days, weeks, months, or years. The pain just gets worse. It can become debilitating. You become desperate for relief, and even that relief doesn’t come without its own consequences.
Chronic pain is the type of pain that many people with fibromyalgia, neuropathic pain, and other complex types of pain suffer from. Normally, the body automatically stops unpleasant sensations like pain. In cases of chronic pain, however, the body’s central nervous system becomes altered, and the body becomes even more sensitive to pain. If this wasn’t bad enough, people with chronic often perceive pain more intensely, where even a gentle touch can be perceived as painful.
Did you know that chemicals released by the body when an injury occurs make changes to the nervous system? These changes can sometimes become unchecked and uncontrolled, compounding the pain process until it reaches an abnormal state. This is the basis of chronic pain.
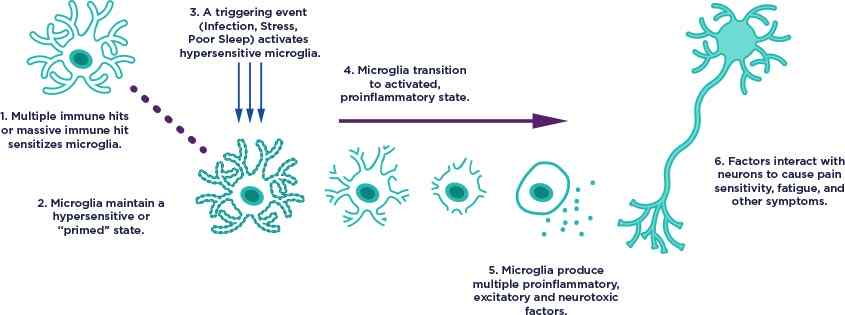
What we’re beginning to learn is that pain may have a lot to do with the gray matter portion of the central nervous system where your brain and spinal cord are located. Until fairly recently, scientists didn’t understand what all of this material was for. Recent research, however, has shed light on certain types of cells in the gray area called Glia. The Glia exist to provide support for all of the nervous system cells and serves various functions. One of the types of glia cells, known as microglia, are responsible for removing bacteria, viruses and dead neurons.
This is where recent research has shed new light on the story of chronic pain. The brain and spinal cord are extremely sensitive areas. As you can imagine, an infection in this part of the body could prove fatal. Microglia in the CNS are especially sensitive to infections and pathological changes. When microglia become activated, they release cellular messengers called cytokines to attract other immune cells to the area, and a complex and intertwined immune process begins to take place. The process leads to inflammation, and if it gets out of hand, chronic inflammation and pain can be an end result.
The current school of thought is that fibromyalgia, complex regional pain syndrome, and neuropathic pain all contain components of this type of microglial cell dysregulation.1-5
Instead of opioids and anti-inflammatory drugs which do not work for these types of condition, physicians usually prescribe anticonvulsants such as gabapentin and pregabalin, or antidepressants like amitriptyline to block various pain pathways. The issue here is that these drugs hardly do more than mask symptoms and are a far cry from treating the root cause. These drugs will never fix what is going on underneath, not to mention that they come with a whole host of their own side effects such as drowsiness, dry mouth, constipation, blurry vision, sexual side effects and a general down feeling. Some, like amitriptyline, must be taken daily and can lead to some very serious side effects if discontinued without tapering.
Fortunately, pain management experts have stumbled onto a unique medication solution called low dose naltrexone. Remarkably, LDN seems to work in a few different ways. We’ll highlight 2 of the pathways that are more defined.
Stated simply, LDN works by blocking the activation of microglia. As mentioned above, microglia are the immune scavengers in the CNS. Due to immune hits and other triggering events, the microglia can become hypersensitized leading to destruction of neurons which can result in pain, sensitivity, and fatigue. Microglia are activated through a certain type of receptor known as the Toll Like Receptor 4 (TLR-4). In the management of pain, naltrexone blocks TLR-4 receptor, thereby preventing and reducing the immune cascade that was causing the symptoms.
The other way in which LDN works is quite paradoxical. Historically, naltrexone has been used as a medication to treat opioid and alcohol addiction. The doses used to treat these conditions, however, are much higher than we would use to treat chronic pain and inflammation. At higher doses, naltrexone persistently blocks an opioid receptor called the opioid growth factor (OGF) receptor. By blocking this receptor, the levels of endorphins and its effects decreases in the body.
In contrast, when naltrexone is used at lower doses, the same OGF receptors are only blocked for a short amount of time. This is where the magic of low dose naltrexone seems to lie. After the initial blockade, the numbers of endorphins, enkephalins, and their receptors skyrocket. The importance of this is that endorphins and enkephalins help to regulate the immune system. There are receptors for endorphins on almost every immune cell in the body. The increase of endorphins and its receptors seems to shift the immune system down a less inflammatory path.
It’s because of these amazing actions that low dose naltrexone has gained some notoriety amongst pain management specialists. It has been used to treat a myriad of painful autoimmune diseases like rheumatoid arthritis and multiple sclerosis. It has also been used with some success in patients who suffer from fibromyalgia6, complex regional pain syndromes7, neuropathic pain including corneal pain8, and chronic lower back pain9.
Low Dose Naltrexone for Fibromyalgia
Low dose naltrexone was administered in trial of 10 women diagnosed with fibromyalgia over a 14-week period. The use of LDN resulted in a reduction in fibromyalgia symptoms severity, as well as significant reductions in pain, fatigue, and stress.6
LDN for Chronic Refractory Lower Back Pain
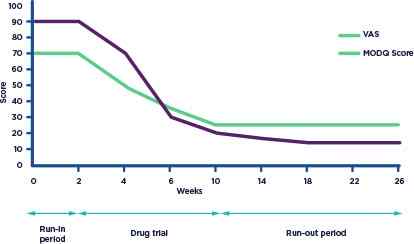
A 35-year-old man had experienced chronic lower back pain for over 2 years. An MRI revealed that he had a bulging disc (at L5-S1). He was previously unsuccessfully treated with tramadol, NSAIDS, amitriptyline, pregabalin, physical therapy, trigger point injections, and steroid injections. His pain score using the visual analog scale (VAS, 0-100 points) was 90-100 most of the time. Needless to say, it interfered with most of his daily activities.

The patient was started on 2mg of LDN for 2 weeks which offered no pain relief. LDN was increased to 4mg for another 2 weeks and he experienced a 30-40% reduction in pain on the new dose. The drug was stopped after 6 weeks, and his pain relief continued. This patient experienced a drastic positive response and was even able to return to work.9
Complex Regional Pain Syndrome (CRPS) – A Case Report
A 2013 case study describes LDN’s positive impact on a young 17-year-old female with the diagnosis of intractable CRPS. The patient presented with a chief complaint of left lower extremity pain rated at an 8/10 (10 being most) on a pain visual analogue scale (VAS).
Despite treatment with gabapentin, ibuprofen, nortriptyline, transdermal clonidine, and trazadone, her pain continued with little relief. LDN was eventually prescribed at 1.5 mg with trazodone. After four weeks, the patient rated her pain on the VAS at 1/10. The patient remained at a dose of 1.5mg LDN.7
Neuropathic Pain – Neuropathic Corneal Pain
Treatment with LDN for corneal pain was presented at the American Academy of Opthamalogy annual meeting. Dieckmann and colleagues conducted a study to determine the efficacy and tolerability of low-dose naltrexone among 30 patients with neuropathic corneal pain. All participants were treated with low-dose naltrexone for at least 4 weeks and answered a questionnaire that evaluated ocular pain and quality of life. All patients were taking previous systemic medications, including nortriptyline and SSRI’s.
Treatment with low-dose naltrexone over reduced mean pain scores by 36.4%, and nearly half of participants (45.5%) showed improvements in pain by at least 50%. Additionally, 12.5% of patients had a positive percentage change in pain scores between 30 and 49.9% and 37.5% of patients improved by less than 30%. Quality of life scores were also improved.8
Low Dose Naltrexone Side Effects
Probably the greatest thing that our pharmacists love about treating patients with LDN is that it doesn’t come with a long list of side effects. In one study, it was shown that low dose naltrexone was just as tolerable as taking a placebo.6 The only side effects noted with LDN are insomnia and vivid dreams. Since most physicians ask their patients to take LDN at night, these side effects can be mitigated by taking it in the morning for a few weeks.
How to Start Low Dose Naltrexone
When starting LDN for pain, most physicians will also ask their patients to start at lower doses than usual, typically 0.5mg. The idea is to increase the dose every week until a sweet spot is found where the greatest amount of pain relief is experienced. Sometimes that means bringing a dose back down. Sometimes, that can mean going beyond the 4.5mg recommended dosage.
LDN and Opiates
Since naltrexone is an opiate blocker, taking it alongside opiates such as hydrocodone or oxycodone may precipitate some withdrawal side effects. While short acting opiates should be avoided within 4 hours of an LDN dose, long acting opiates should be avoided altogether. If any opiates are taken with LDN, this should be under the strict care of a physician.
How to Get Low Dose Naltrexone: Pain Management Doctors
If you’re interested in a trial of LDN, look no further. We work with a group of physicians who you can reach out to for help right away. Many may be available to see you through a simple and quick telemedicine visit.
Give us a call today at:
(949) 642-0106 and get a LDN physician referral to start your path towards pain relief!
